
Venous and Arterial Thrombosis Risk Testing - CAM 283
Description
A thrombosis, also known as a blood clot, occurs within blood vessels in the body. The two main types of thrombosis include venous thrombosis, which is when a vein is blocked due to a blood clot, and arterial thrombosis, which is when an artery is blocked due to a blood clot. Thrombophilias refer to hereditary and/or acquired abnormalities of hemostasis that predispose patients to thrombosis.1 The most common presentations of venous thromboembolism (VTE) are deep vein thrombosis (DVT) and pulmonary embolism (PE).2
Terms such as male and female are used when necessary to refer to sex assigned at birth.
Regulatory Status
A search for “thrombosis” on the FDA website yielded 12 results on January 26, 2021 (FDA, 2021). Many labs have developed specific tests that they must validate and perform in house. These laboratory-developed tests (LDTs) are regulated by the Centers for Medicare & Medicaid Services (CMS) as high-complexity tests under the Clinical Laboratory Improvement Amendments of 1988 (CLIA ’88). As an LDT, the U.S. Food and Drug Administration has not approved or cleared this test; however, FDA clearance or approval is not currently required for clinical use.
Policy
Application of coverage criteria is dependent upon an individual’s benefit coverage at the time of the request.
- For individuals without recurrent venous thromboembolism (VTE) risk factors (e.g., surgery, prolonged immobilization, collagen vascular disease, malignancy, certain hematologic disorders), genetic testing for Factor V Leiden and prothrombin gene G20210A mutations and plasma testing for protein C deficiency, protein S deficiency, and antithrombin III deficiency (see Note 1) is considered MEDICALLY NECESSARY in any of the following situations:
- For individuals less than 50 years of age who have experienced any deep venous thrombosis (DVT) or pulmonary embolism (PE).
- For individuals who have experienced a DVT in unusual sites (e.g., hepatic, mesenteric, or cerebral veins).
- For individuals who have experienced a DVT and who have a strong family history of thrombotic disease.
- For individuals who have experienced a DVT and who are pregnant or who are taking oral contraceptives (OCs).
- For first- and second-degree relatives (see Note 2) of individuals who experienced a DVT before 50 years of age.
- Before the administration of oral contraceptives, targeted testing of individuals with a personal or family history of DVT.
- For pediatric individuals who have suffered from a pediatric arterial ischemic stroke.
- For individuals with warfarin-induced skin necrosis or for infants who develop neonatal purpura fulminans, plasma testing for protein C deficiency and protein S deficiency (see Note 1) is considered MEDICALLY NECESSARY.
- For individuals who are contemplating estrogen use (OCs or hormone replacement therapy) and who have a first-degree relative (see Note 2) with a known Factor V Leiden or prothrombin gene G20210A mutation, genetic testing for the known familial mutation is considered MEDICALLY NECESSARY.
- For hypercoagulable evaluation or for “at risk” family members, MTHFR genetic testing is considered NOT MEDICALLY NECESSARY.
- For individuals with recurrent thrombotic events who are receiving a lifelong anticoagulation regimen, genetic testing for Factor V Leiden and prothrombin gene G20210A mutations is considered NOT MEDICALLY NECESSARY.
- Venous thrombosis risk testing for superficial venous thrombosis (including superficial thrombophlebitis and varicosities) is considered NOT MEDICALLY NECESSARY.
- For all situations, activated protein C (aPC) resistance assay is considered NOT MEDICALLY NECESSARY.
The following does not meet coverage criteria due to a lack of available published scientific literature confirming that the test(s) is/are required and beneficial for the diagnosis and treatment of an individual’s illness.
- Genetic testing for inherited thrombophilia is considered NOT MEDICALLY NECESSARY for any of the following situations:
- For the evaluation of recurrent fetal loss, placental abruption, preeclampsia, or fetal growth restriction.
- For the evaluation of arterial thrombosis not attributable to paradoxical emboli.
- As a routine screen for the general population.
- As a routine screen for asymptomatic individuals considering oral contraceptive use or hormone replacement therapy.
- As a routine screen for asymptomatic pregnant individuals.
- For prenatal or preimplantation testing.
- As a routine newborn screen.
- Genetic testing for inherited thrombophilia more than once per lifetime is considered NOT MEDICALLY NECESSARY.
- Testing for other genetic thrombophilia risk factors (e.g., factor V HR2 variant, prothrombin G1199A variant, factor VII R353Q variant, factor 13B V34L variant, PAI-1), as well as multi-gene panel testing is considered NOT MEDICALLY NECESSARY.
- DVT risk testing as part of a pre-transplant evaluation test is considered NOT MEDICALLY NECESSARY.
- To determine arterial thrombosis risk, genetic testing for Factor V Leiden mutation and prothrombin gene G20210A mutation is considered NOT MEDICALLY NECESSARY.
NOTES:
Note 1: Psmlaa testing for protein C deficiency, protein S deficiency, and antithrombin III deficiency should be performed at least six weeks after the acute thrombotic event and while the patient is not taking anticoagulants.
Note 2: First-degree relatives include parents, full siblings, and children of the individual. Second-degree relatives include grandparents, aunts, uncles, nieces, nephews, grandchildren, and half-siblings of the individual.
Table of Terminology
| Term |
Definition |
| ACC |
American College of Cardiology |
| ACMG |
American College of Medical Genetics and Genomics |
| ACOG |
American College of Obstetricians and Gynecologists |
| ACR |
American College of Radiology |
| AHA/ASA |
American Heart Association/American Stroke Association |
| aPC |
Activated protein C |
| APS |
Antiphospholipid syndrome |
| ASCP |
American Society for Clinical Pathology |
| ASH |
American Society of Hematology |
| COC |
Combined oral contraceptives |
| CTPA |
Computed tomography pulmonary angiography |
| DVT |
Deep vein thrombosis |
| EGAPP |
Evaluation of genomic applications in practice and prevention |
| ESC |
European Society of Cardiology |
| FVL |
Factor V Leiden |
| GAHT |
Gender-affirming hormone therapy |
| HRT |
Hormone replacement therapy |
| NAFT |
The North American Thrombosis Forum |
| OC |
Oral contraceptives |
| PE |
Pulmonary embolism |
| PERC |
Pulmonary Embolism Rule-out Criteria |
| PGM |
Prothrombin 20210A gene mutation |
| SIGN |
Scottish Intercollegiate Guidelines Network |
| SPESI |
Simplified pulmonary embolism severity index |
| SVM |
Society for Vascular Medicine |
| VQ |
Ventilation perfusion |
| VTE |
Venous thromboembolism |
| VUS |
Variant of unknown significance |
Rationale
A thrombus is “an aggregate of coagulated blood within the vascular system or heart which contains platelets, fibrin, leukocytes, and red blood cells in varying amounts.”3 This aggregate of blood can be problematic as it may obstruct normal blood circulation throughout the body and even travel to peripheral areas. The primary manifestations of venous thromboembolisms (VTE) are deep vein thrombosis and pulmonary embolism. These conditions affect an estimated one million individuals in the United States annually.2
Thrombosis is widely theorized to develop due to Virchow’s Triad, which consists of abnormalities in blood flow, a vascular endothelial injury, and alterations in the blood constituents. Changes in any of these characteristics may cause the clot to form.4 For example, sickle red blood cells may cause increased clumping or decreased adhesion to the vessel walls.5 There are two main types of thrombosis: venous thrombosis (when a vein is blocked due to a blood clot) and arterial thrombosis (when an artery is blocked due to a blood clot).
A deep vein thrombosis (DVT) refers to a thrombus in a “deep” vein whereas a pulmonary embolism (PE) refers to an obstruction of the pulmonary artery (or one of its branches) by foreign material. 6,7 DVT of the lower extremities may cause symptoms, such as swelling or edema in the lower extremities, pain, and warmth in the affected area.6 This thrombus may travel to the lungs (becoming an embolus) and cause a PE. A PE has similar symptoms to DVT but may include pulmonary issues, such as shortness of breath. The risk factors for VTE, PE, and DVT are similar. 7 The two primary categories of risk factors for VTE are hereditary and acquired, and the genetic tendency toward VTE is referred to as inherited thrombophilia. Hereditary risk factors include genetic mutations such as Factor V Leiden (FVL) mutations. The five most common genetic risk factors for VTE are FVL mutations, prothrombin mutations, protein S defect, protein C defect, and antithrombin defect.4 Approximately 50–60% of the variance in VTE incidence are attributed to genetic effects.8
A modified activated partial thromboplastin time (aPTT) assay detects the anticoagulant activity of activated protein C (aPC). FVL mutations cause coagulation factor V to be unresponsive to aPC and initially, these changes were termed “aPC resistance” due to the reduced activity of aPC on a modified aPTT assay. A single nucleotide change (G1691A) results in a point mutation of glutamine to arginine at position 506. Approximately 99% of carriers of this mutation are heterozygous, and only five percent of these heterozygotes will experience a VTE in their lifetime. These mutations are often suspected in patients experiencing a VTE at a young age (under 50), a VTE in unusual areas such as a portal vein, or recurrent VTEs.9 Protein C may also be genetically deficient, but this mutation is only seen in two to five percent of individuals with a VTE.6 Protein S, a cofactor for the aPC control mechanism, and deficiencies in this protein may also confer additional risk for VTE.10
The second most common inherited thrombophilia is the G20210A mutation of prothrombin. This mutation is a gain of function mutation where clotting activity is increased by creating more thrombin and fibrin. The overall prevalence of this mutation is about two percent.11 Genetic defects of antithrombin (an inhibitor of thrombin) may also occur, but the estimated prevalence of antithrombin defects is only a maximum of 0.2%.12
Acquired risk factors or predisposing conditions for thrombosis include a prior thrombotic event, recent major surgery, presence of a central venous catheter, trauma, immobilization, malignancy, pregnancy, the use of oral contraceptives or heparin, myeloproliferative disorders, antiphospholipid syndrome (APS), and a number of other major medical illnesses.4 Patients with acquired hypercoagulability have an increased risk of venous thrombosis, arterial thrombosis, or both; however, there is a low-risk of recurrence, regardless of thrombophilia status.13 A rare complication of warfarin treatment, warfarin-induced skin necrosis is commonly due to protein C deficiency, with rare cases of protein S deficiency or PVL having been reported.14
Risk factors for arterial thrombosis are lesser known. The relationship between FVL and arterial thrombosis is controversial with studies reporting varying results; overall, FVL is not currently considered a major risk factor for arterial thrombosis.15,16 Kujovich (2018) states that FVL testing should not be performed on persons with any type of arterial thrombosis including myocardial infarction and stroke in children or adults. It has also been reported that while inherited antithrombin, protein S and protein C deficiencies are important risk factors for venous thrombosis, “they have little or no effect on arterial thrombosis.”18 Further, prothrombin gene mutation is not consistently shown to increase the risk of an arterial thromboembolism, and “There is no association of antithrombin deficiency with arterial thrombosis.”16
It has been proposed that venous thrombosis risk testing may be beneficial as a pre-transplant evaluation test. However, no studies have been identified suggesting this. The North American Thrombosis Forum (NAFT) states that even though certain genetic conditions predispose a small proportion of the population to the development of blood clots, “few people with thrombophilias develop symptoms”; further, there is no cost-effective, safe or long-term method to prevent a blood clot from forming even if a genetic predisposition is identified.19
Thrombotic events such as thrombophilia and stroke have become increasingly documented in hospitalized pediatric patients with underlying medical conditions such as prematurity, cancer, and congenital heart disease, but they are rarely identified in healthy children. Furthermore, in most cases of pediatric venous thromboembolism, there exist other underlying risk factors such as indwelling central venous catheter and inherited thrombophilia that are worthy of further investigation. The incidence of venous thromboembolisms is highest in neonates and infants, but there is a second peak recorded in adolescence, coinciding with the use of oral contraceptives. However, as in the case with adults, little to no evidence suggests that the use of venous thrombosis risk testing in children will affect the acute management of venous thromboembolisms. In a study including a total of 271 children with VTE, it was found that the relative frequencies of individually inherited thrombophilias were low—for example, the highest recorded frequency of IT disorders was of Factor V Leiden, occurring in only five to ten percent of the samples. Moreover, a study of 52 children with thromboembolic events during the acute phase did not urge any changes to acute management, regardless of the result of the test.20
Venous thrombosis risk testing has also been entertained as a manner of combatting pediatric stroke, which can be characterized in a variety of ways, such as by age and by presentation. Arterial ischemic infarctions are the most common, comprising approximately 80% of all perinatal strokes, and this form of stroke can occur in up to one in 3500 of newborns. However, though it would seem reasonable for venous thrombosis risk testing to be employed here, recent prospective case-control studies suggest that routine thrombophilia testing is not warranted. The study showed that conditions associated with thrombophilia rarely coincided with arterial ischemic strokes, and these conditions included, but were not limited to, decreased levels of protein C, protein S, or prothrombin, and genotyping of FVL and factor II (FII, prothrombin) G20210A. Of the 14 parameters examined, 12 showed no difference, including all common thrombophilias examined, with specific mention that FVL and FII were comparable to population norms.21,22 Subsequent evaluation deemed thrombophilia evaluation in neonates as having limited clinical utility because “levels of protein C, protein S, antithrombin, and factor XI are normally decreased to 30% of adults levels, and these levels only approach adult levels at various time points during childhood.” Therefore, the use of thrombophilia testing for these proteins may be misleading in the neonatal period, and MRIs instead should be used to diagnose the thrombosis.22 Moreover, studies focusing on the roles of thrombophilia, arteriopathy, and cardiac abnormalities in perinatal ischemic stroke find that these risk factors were at best unclear, weakening what predictive power they were believed to contain for even recurrent events after perinatal stroke and leading researchers to conclude that thrombophilia evaluation should rarely be considered in cases of perinatal stroke.23
While the initial aPTT assays used unaltered plasma (first-generation assays), some versions were neither sensitive nor specific for FVL. Modifications to this test resulted in second generation functional aPC resistance assays that correlate well with the presence of FVL. However, in rare cases, functional assays for aPC resistance can give misleading results (e.g., the presence of a lupis anticoagulant can cause falsely abnormal results in some assays; therapy with a direct thrombin inhibitor or oral factor Za inhibitor can cause falsely normal results). In addition, while FVL can be detected by genetic testing or a second-generation functional coagulation test for aPC resistance, individuals with a positive aPC resistance assay would still need to receive genetic testing to confirm a diagnosis.9 Due to difficulty with interpretation, a need for confirmatory genetic testing, and the overall declining cost of genetic testing, aPC resistance assays are performed infrequently. When performed, they are simply reported as positive, borderline, or negative.9
The term FVL paradox describes the different risk of DVT and PE in FVL carriers; there is data to suggest that FLV carriers are less likely to experience isolated PE (without DVT) than the general population.9 de Moerloose, et al. (2000) studied the prevalence of FVL in people suspected of DVT and/or PE. The 99 participants with PE were categorized based on “those with PE but without DVT (n = 57) and those with PE and DVT (n = 42).” The odds ratio for the prevalence of FVL was higher (19.1%) in patients with DVT and PE than the odds ratio for the prevalence of FVL in patients with only PE (10.5%), suggesting that “patients with primary PE are less often affected by the factor V Leiden mutation.” In another study by Mäkelburg, et al. (2010), the relative risk of DVT in FVL carriers compared to non-carriers was 7.0, while the relative risk of PE in FVL carriers compared to non-carriers was 2.8.
Analytical Validity
Murphy and Sabath (2019) have compared the accuracy and reliability of two tests: a genotypic assay which identifies FVL mutations, and a phenotypic aPC resistance assay. Data from 1596 patients was analyzed; each patient had received both types of testing. The authors state that the phenotypic testing exhibited both high sensitivity and specificity compared to genotypic testing. “Phenotypic assays had close to total concordance with genotypic assays over 16 years of testing. Changing ordering practices could result in up to an 80% reduction in testing costs.”26
A systematic review and meta-analysis by Chiasakul, et al. (2019) researched the relationship between inherited thrombophilia and the risk of arterial ischemic stroke in adults. Inherited thrombophilias included FVL, protein C and S deficiency, antithrombin deficiency and prothrombin G20210A mutation. For this study, 11,916 stroke patients and 96,057 controls were identified. The authors concluded that “Compared with controls, patients with arterial ischemic stroke were significantly more likely to have the following inherited thrombophilias: factor V Leiden (OR, 1.25; 95% CI, 1.08-1.44; I2=0%), prothrombin G20210A mutation (OR, 1.48; 95% CI, 1.22-1.80; I2=0%), protein C deficiency (OR, 2.13; 95% CI, 1.16-3.90; I2=0%), and protein S deficiency (OR, 2.26; 95% CI, 1.34-3.80; I2=8.8%).”27 Antithrombin deficiency did not reach statistical significance in this study. Hence, in this review, inherited thrombophilias were found to be associated with an increased risk of arterial ischemic stroke in adults.
In a systematic review, Ordieres-Ortega, et al. (2020) studied the predictive value of D-dimer testing for venous thrombosis diagnosis in unusual locations. A total of 3378 patients from 23 articles with thrombosis in unusual sites, such as upper extremity DVT, cerebral vein thrombosis (CVT) and splanchnic vein thrombosis (SVT), were studied. Twelve articles on CVT concluded that timing of D-dimer testing is important and patients with short duration of symptoms displayed higher D-dimer levels. Sensitivity and specificity in these patients ranged from 58% to 97% and from 77% to 97.5%, respectively. The authors conclude that "D-dimer testing should not be currently recommended for the diagnosis of thrombosis in unusual sites as a first line diagnostic tool. The development of algorithms combining biomarkers such as D-dimer and clinical decision tools could improve the diagnosis.”28
Clinical Utility and Validity
A D-dimer assay is a blood test that is used in clinical practice to assist in identifying if a patient has a DVT or PE; this test may also help patients experiencing unprovoked VTE to determine if anticoagulation treatment should continue or halt after initial treatment is complete.29 A D-dimer assay may vary greatly based on the type of antibody used, the method of capture, calibration, and instrumentation. Currently, 30 different assays as available which use 20 different monoclonal antibodies; various studies have reported a broad sensitivity and specificity range for D-dimer assays from 69-97% and 43-99% respectively.29 Hence, all D-dimer assays differ and need to be validated within the population of interest. Because of this, comparing study results is challenging.
Factor VIII is a blood clotting protein encoded by the F8 gene. A case report by Algahtani and Stuckey (2019) suggests that high factor VIII levels may also assist in risk factor determination for thrombosis or ischemic heart disease. “We conclude that high factor VIII levels are a risk factor for thrombosis, with a greater impact on venous than on arterial thrombosis. However, due to a lack of international consensus on methods for the laboratory testing of factor VIII levels in plasma, we would not currently recommend the measurement of factor VIII levels as part of routine thrombophilia screening.”30 This relationship has been shown previously as elevated levels of coagulation factor VIII:C were identified in a retrospective study of 584 first-degree relatives of 177 patients with high coagulation factor VIII:C levels; the researchers found that 40% of first-degree relatives also had high VIII:C levels and were at an increased risk for VTE and arterial thrombosis when compared to other first-degree relatives with normal VIII:C levels.31
Lee, et al. (2017) performed whole exome sequencing on 64 patients with VTE to assess the types of mutations of inherited thrombophilias. Of these 64 patients, 39 of them were found to have a pathogenic variant or variant of unknown significance (VUS). Further, eight were found to have a Factor V mutation (six with FVL and two with less common mutations), two were found to have a prothrombin G20210A mutation, six were found to have a protein S mutation, two were found to have a protein C mutation, and three were found to have an antithrombin mutation.32
Segal, et al. (2009) reviewed the utility of FVL and prothrombin G20210A testing. The authors reviewed 124 articles and concluded that although genetic testing for these two risk factors is very accurate (valid), the clinical utility is lacking due to lack of evidence demonstrating improvement in clinical outcomes.33
Onda, et al. (2021) studied the clinical utility of a new diagnostic algorithm based on serum D-dimer levels for VTE after hepatectomy. A total of 742 patients who underwent hepatectomy were enrolled in the study and measured for serum D-dimer levels post-op. CT scan was performed for patients who had a D-dimer level of greater than 20 μg/mL. Based on D-dimer and CT scan, VTE was diagnosed in 26 patients and PE was diagnosed in 18 patients. Multivariate analysis also showed that a resected liver weight of more than 120 grams is a significant predictor of VTE. Overall, “patients who undergo hepatectomy are at high risk for VTE, especially when the resected liver weight is high. The proposed diagnostic algorithm based on serum D-dimer levels for VTE after hepatectomy can be useful for early diagnosis."34
American Heart Association/American Stroke Association (AHA/ASA)
The AHA/ASA has issued a scientific statement for the management of stroke in neonates and children, wherein testing for thrombophilic abnormalities are discussed. The AHA/ASA admits that due to the lack of “an adequately powered study to detect the impact of genetic thrombophilia on recurrence risk in pediatric AIS [arterial ischemic stroke], definite recommendations about evaluation remain challenging”, but acknowledges that “laboratory testing outside of clinical studies may provide guidance for long-term management of the patient.” For cases of thrombophilia the AHA/ASA provides an algorithm for the “Targeted Evaluation of a Child With AIS for Rare Causes or Causes Requiring Additional Evaluation” that includes the examination of Factor VIII level, Lipoprotein(a), MTHFR mutation, and homocysteine levels, and it is suggested that “non-DNA testing may need to be repeated when the child is older to ensure that adult levels of proteins have been attained” and “measurement of proteins or homocysteine levels in the acute phase of stroke may not be accurate and should be repeated after the acute event.” Finally, for the evaluation of a child with AIS, it is believed that “a thrombophilia evaluation is helpful in every case of childhood stroke, especially if there is no identifiable cause, medical history of thrombosis, or a first-degree relative with thrombosis history.”22
In 2021, the AHA released guidelines on stroke prevention. The AHA brushes on testing for hematologic traits in the context of secondary stroke prevention. "If in certain clinical scenarios (eg, paradoxical emboli caused by venous thrombosis or recurrent venous thrombosis) testing for thrombophilic states is considered, testing for protein C, protein S, or antithrombin levels should be deferred or repeated at least 4 to 6 weeks (or up to 6 months for factor VIII609) after the acute stroke given that these protein levels may be altered during the acute stroke phase.”35
American College of Medical Genetics and Genomics (ACMG)
The ACMG has released guidelines, which incorporate several recommendations and suggestions from the American Society of Hematology, for laboratory testing of venous thromboembolism (VTE). Testing for Factor V Leiden and factor II c.*97G>A (this mutation is also known as G20210A) is recommended in the following circumstances:
- “VTE at unusual sites (such as cerebral and splanchnic venous thrombosis)
- for individuals with VTE provoked by pregnancy or postpartum
- for individuals with VTE associated with the use of OCs
- personal history of VTE with (a) a positive family history of thrombophilia diagnosed in a first- or second-degree relative or (b) 1 first-degree relative with VTE at a young age
- individuals with low APC resistance activity
Testing may be considered in the following circumstances:
- recurrent VTE
- siblings of individuals known to be homozygous for FVL or factor II c.∗97G>A
- asymptomatic pregnant individual or individual contemplating pregnancy or estrogen use (OC or hormone replacement therapy) who has a first-degree relative with a history of VTE and is known to be homozygous FVL or is double heterozygotes of FVL and factor II c.97∗G>A variant
- asymptomatic pregnant individual or individual contemplating pregnancy with a previous nonestrogen-related VTE or VTE provoked by a minor risk factor because knowledge of the FVL and/or factor II c.∗97G>A status may alter pregnancy-related thrombophylaxis36
The ACMG found several clinical scenarios requiring special considerations worth mentioning, involving different populations. One involved the testing of asymptomatic versus symptomatic individuals, in which they assert that “it is generally not recommended to test asymptomatic minors as VTE rarely occurs before young adulthood even in the homozygous state.” For prenatal testing and population screening, the ACMG suggests that “prenatal testing and population screening are not indicated due to the low penetrance of these variants, later age of onset, and lack of genotype-directed prophylaxis.” Lastly, in individuals considering taking estrogen-containing oral contraceptives (OC) or hormone replacement therapy (HRT), the ACMG indicates that “a family and personal history of thrombosis should be carefully evaluated for all women before initiating HRT and a positive history may warrant thrombophilia screening.”37
The ACMG does not support testing for MTHFR variants in thrombophilia assessment due to the lack of correlation with negative pregnancy outcomes.38 This statement was reaffirmed in 2020 and 2025.36,39
American Society of Hematology (ASH)
The 2013 ASH recommends against testing “for thrombophilia in adult patients with venous thromboembolism (VTE) occurring in the setting of major transient risk factors (surgery, trauma or prolonged immobility).”40
In 2018, ASH released their guidelines for management of venous thromboembolism, which included the following recommendations.41 These guidelines were reviewed in 2022 by an ASH expert working group and agreed to “continue monitoring the supporting evidence rather than revise or retire these guidelines at this time.”
- “Recommends using a strategy starting with D-dimer for excluding PE in a population with low prevalence/PTP (≤5%), followed by ventilation-perfusion (VQ) scan or computed tomography pulmonary angiography (CTPA) for patients requiring additional testing.
- Recommends against using a positive D-dimer alone to diagnose PE, and against additional testing following negative CTPA or normal VQ scan in a population with low prevalence/PTP (≤5%).
- Suggests using a strategy starting with D-dimer for excluding PE in a population with intermediate prevalence/PTP (∼20%), followed by VQ scan or CTPA for patients requiring additional testing.
- Recommends against using a positive D-dimer alone to diagnose PE, and against additional testing following negative CTPA or normal VQ scan in a population with intermediate prevalence/PTP (∼20%).
- Recommends against using a positive D-dimer alone to diagnose PE, and against using D-dimer as a subsequent test following a negative CT scan in a population with high prevalence/PTP (≥50%).
- Suggests using a strategy starting with D-dimer for excluding recurrent PE in a population with unlikely PTP.
- Recommends using a strategy starting with D-dimer for excluding DVT in a population with low prevalence/PTP (≤10%), followed by proximal lower extremity ultrasound or whole-leg ultrasound for patients requiring additional testing.
- Recommends against using a positive D-dimer alone to diagnose DVT, and against additional testing following negative proximal or whole-leg ultrasound in a population with low prevalence/PTP (≤10%).
- Recommends against using a positive D-dimer alone to diagnose DVT in a population with intermediate prevalence/PTP (∼25%).
- Recommends against using a positive D-dimer alone to diagnose DVT in a population with high prevalence/PTP (≥50%).
- Suggests using a strategy starting with D-dimer for excluding recurrent DVT in a population with unlikely PTP.
- Suggests a strategy starting with D-dimer for excluding upper extremity DVT in a population with low prevalence/unlikely PTP (10%), followed by duplex ultrasound if D-dimer is positive.
- Recommends against using a positive D-dimer alone to diagnose upper extremity DVT in a population with low prevalence/unlikely PTP (10%).
- Suggests a strategy of either D-dimer followed by duplex ultrasound/serial duplex ultrasound, or duplex ultrasound/serial duplex ultrasound alone for assessing patients suspected of having upper extremity DVT in a population with high prevalence/likely PTP (40%).
- Recommends against using a positive D-dimer alone to diagnose upper extremity DVT in a population with high prevalence/likely PTP (40%).”41
In 2020, the ASH released guidelines on management of venous thromboembolism. ASH suggest “against the routine use of prognostic scores, D-dimer testing, or venous ultrasound to guide the duration of anticoagulation.”42 These guidelines were reviewed by an expert work group convened by ASH in August of 2022.
In 2023, the ASH released guidelines thrombophilia testing for the management of venous thromboembolism. “The panel issued a strong recommendation against testing the general population before starting combined oral contraceptives (COCs) and conditional recommendations for thrombophilia testing in the following scenarios: (a) patients with VTE associated with nonsurgical major transient or hormonal risk factors; (b) patients with cerebral or splanchnic venous thrombosis, in settings where anticoagulation would otherwise be discontinued; (c) individuals with a family history of antithrombin, protein C, or protein S deficiency when considering thromboprophylaxis for minor provoking risk factors and for guidance to avoid COCs/hormone replacement therapy; (d) pregnant women with a family history of high-risk thrombophilia types; and (e) patients with cancer at low or intermediate risk of thrombosis and with a family history of VTE. For all other questions, the panel provided conditional recommendations against testing for thrombophilia.” The panel also listed the following 23 recommendations:43
- “For patients with unprovoked VTE who have completed primary short-term treatment, the ASH guideline panel suggests not to perform thrombophilia testing to guide the duration of anticoagulant treatment (conditional recommendation based on very low certainty in the evidence about effects).”
- “For patients with VTE provoked by surgery who have completed primary short-term treatment, the ASH guideline panel suggests not to perform thrombophilia testing to determine the duration of anticoagulant treatment (conditional recommendation based on very low certainty in the evidence about effects).”
- “For patients with VTE provoked by a nonsurgical major transient risk factor who have completed primary short-term treatment, the ASH guideline panel suggests testing for thrombophilia to guide anticoagulant treatment duration. The panel suggests indefinite anticoagulant treatment for patients with thrombophilia and stopping anticoagulant treatment for patients without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women with VTE provoked by pregnancy or postpartum who have completed primary treatment, the ASH guideline panel suggests thrombophilia testing to guide anticoagulant treatment duration. The panel suggests indefinite anticoagulant treatment for women with thrombophilia and stopping anticoagulant treatment for women without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women with VTE associated with COCs who have completed primary short-term treatment, the ASH guideline panel suggests testing for thrombophilia to guide anticoagulant treatment duration. The panel suggests indefinite anticoagulant treatment for women with thrombophilia and stopping anticoagulant treatment for women without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For patients with an unspecified type of VTE who have completed primary short-term treatment, the ASH guideline panel suggests not performing thrombophilia testing to guide anticoagulant treatment duration (conditional recommendation based on very low certainty in the evidence about effects).”
- “For patients with CVT who have completed primary treatment in a setting where anticoagulation would be discontinued, the ASH guideline panel suggests thrombophilia testing to guide anticoagulant treatment duration. The panel suggests indefinite anticoagulation for patients with thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For patients with CVT who have completed primary treatment in a setting where anticoagulation would be continued indefinitely, the ASH guideline panel suggests not to perform thrombophilia testing to guide anticoagulant treatment duration (conditional recommendation based on very low certainty in the evidence about effects).”
- “For patients with splanchnic venous thrombosis who have completed primary treatment in a setting where anticoagulation would be discontinued, the ASH guideline panel suggests thrombophilia testing to guide anticoagulant treatment duration. The panel suggests indefinite anticoagulation for patients with thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For patients with splanchnic venous thrombosis who have completed primary treatment in a setting where anticoagulation would be continued indefinitely, the ASH guideline panel suggests not performing thrombophilia testing to guide anticoagulant treatment duration (conditional recommendation based on very low certainty in the evidence about effects).”
- “For individuals with a family history of VTE and known FVL or PGM [prothrombin 20210A gene mutation] (low-risk thrombophilia) who have a minor provoking risk factor for VTE (eg, immobility or minor injury, illness, or infection), the ASH guideline panel suggests not testing for the known familial thrombophilia to guide thromboprophylaxis (conditional recommendation based on very low certainty in the evidence about effects). For individuals with a family history of VTE and known antithrombin, protein C, or protein S deficiency (high-risk thrombophilia) who have a minor provoking risk factor for VTE, the ASH guideline panel suggests testing for the known familial thrombophilia. The panel suggests thromboprophylaxis in individuals with thrombophilia and no thromboprophylaxis in individuals without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For individuals with a family history of VTE and known FVL or PGM (low-risk thrombophilia) who have a minor provoking risk factor for VTE (eg, immobility or minor injury, illness, or infection), the ASH guideline panel suggests not testing for all hereditary thrombophilias to guide thromboprophylaxis (conditional recommendation based on very low certainty in the evidence about effects). For individuals with a family history of VTE and known antithrombin, protein C, or protein S deficiency (high-risk thrombophilia) who have a minor provoking risk factor for VTE, the ASH guideline panel suggests testing for all hereditary thrombophilias (using a panel of tests). The panel suggests thromboprophylaxis in individuals with thrombophilia and no thromboprophylaxis for a minor provoking risk factor in individuals without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For individuals with a family history of VTE and unknown thrombophilia status in the family who have a minor provoking risk factor for VTE (eg, immobility or minor injury, illness, or infection), the ASH guideline panel suggests not testing for all hereditary thrombophilias (using a panel of tests) to guide thromboprophylaxis (conditional recommendation based on very low certainty in the evidence about effects).”
- “For individuals with a family history of FVL or PGM (low-risk thrombophilia) but no family history of VTE who have a minor provoking risk factor for VTE (eg, immobility or minor injury, illness, or infection), the ASH guideline panel suggests not testing for the known thrombophilia to guide thromboprophylaxis (conditional recommendation based on very low certainty in the evidence about effects). For individuals with a first-degree family history of antithrombin, protein C, or protein S deficiency (high-risk thrombophilia) but no family history of VTE who have a minor provoking risk factor for VTE, the ASH guideline panel suggests testing for the known thrombophilia. The panel suggests thromboprophylaxis in individuals with thrombophilia and no thromboprophylaxis in individuals without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects). For individuals with a second-degree family history of antithrombin, protein C, or protein S deficiency (high-risk thrombophilia) but no family history of VTE who have a minor provoking risk factor for VTE, the ASH guideline panel suggests either testing for the known thrombophilia or not testing for thrombophilia to guide the use of thromboprophylaxis (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women from the general population who are considering using COCs, the ASH guideline panel recommends not performing thrombophilia testing to guide the use of COC (strong recommendation based on low certainty in the evidence about effects).”
- “For women from the general population who are considering using HRT, the ASH guideline panel suggests not performing thrombophilia testing to guide the use of HRT (conditional recommendation based on low certainty in the evidence about effects).”
- “For women with a family history of VTE and unknown thrombophilia status in the family who are considering using COCs, the ASH guideline panel suggests not testing for hereditary thrombophilia (using a panel of tests) to guide the use of COC (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women with a family history of VTE and unknown thrombophilia in the family who are considering using HRT, the ASH guideline panel suggests not performing thrombophilia testing for any hereditary thrombophilia to guide the use of HRT (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women with a family history of VTE and known FVL or PGM in the family (low-risk thrombophilia), the ASH guideline panel suggests not testing for the known familial thrombophilia to guide the use of COC (conditional recommendation based on very low certainty in the evidence about effects). For women with a family history of VTE andknown antithrombin, protein C, or protein S deficiency in the family (high-risk thrombophilia), the ASH guideline panel suggests testing for the known familial thrombophilia. The panel suggests avoidance of COCs for women with high-risk thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women with a family history of VTE and known FVL or PGM in the family (low-risk thrombophilia), the ASH guideline panel suggests not testing for the known familial thrombophilia to guide the use of HRT (conditional recommendation based on very low certainty in the evidence about effects). For women with a family history of VTE and known antithrombin, protein C, or protein S deficiency in the family (high-risk thrombophilia), the ASH guideline panel suggests testing for the known familial thrombophilia. The panel suggests avoidance of HRT for women with high-risk thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women with a family history of VTE and known homozygous FVL, a combination of FVL and PGM, or an antithrombin deficiency in the family, the ASH guideline panel suggests testing for the known familial thrombophilia. The panel suggests antepartum thromboprophylaxis for women with the same familial thrombophilia (ie, homozygous FVL, combination of FVL and PGM, or antithrombin deficiency) and no antepartum prophylaxis for women without the same familial thrombophilia (conditional recommendation based on very low certainty in the evidence about effects). For women with a family history of VTE and a known protein C or protein S deficiency in the family, the ASH guideline panel suggests either testing for the known familial thrombophilia or not testing for thrombophilia to guide antepartum prophylaxis (conditional recommendation based on very low certainty in the evidence about effects).”
- “For women with a first-degree family history of VTE and known homozygous FVL, a combination of FVL and PGM, antithrombin deficiency, protein C deficiency, or protein S deficiency in the family, the ASH guideline panel suggests testing for the known familial thrombophilia. The panel suggests postpartum thromboprophylaxis for women with the same familial thrombophilia (ie, homozygous FVL, combination of FVL and PGM, or antithrombin deficiency) and no postpartum prophylaxis for women without the same familial thrombophilia (conditional recommendation based on very low certainty in the evidence about effects). For women with a second-degree family history of VTE and a known combination of FVL and PGM, or antithrombin deficiency in the family, the ASH guideline panel suggests testing for the known familial thrombophilia. The panel suggests postpartum thromboprophylaxis for women with thrombophilia and no postpartum prophylaxis for women without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects). For women with a second-degree family history of VTE and a known protein C or protein S deficiency in the family, the ASH guideline panel suggests either testing for the known familial thrombophilia or not testing for thrombophilia to guide postpartum thromboprophylaxis (conditional recommendation based on very low certainty in the evidence about effects).”
- "For ambulatory patients with cancer receiving systemic therapy who have a family history of VTE and are otherwise determined to be at low or intermediate risk for VTE, the ASH guideline panel suggests testing for hereditary thrombophilia. The panel suggests ambulatory thromboprophylaxis for patients with thrombophilia and no thromboprophylaxis for patients without thrombophilia (conditional recommendation based on very low certainty in the evidence about effects).”43
In a 2024 educational report, the American Society of Hematology (ASH) cautions that gender-affirming hormone therapy (GAHT), particularly estrogen-based therapy, has been associated with thrombotic complications. The report notes well-documented evidence that “oral estrogen elevates systemic levels of clotting factors II, VII, VIII, and X and fibrinogen, decreases the levels of antithrombin and protein S, and induces an acquired resistance to activated protein C in cisgender women. A recent study observed similar changes in procoagulant markers in transgender and gender diverse individuals receiving an oral estrogen formulation.” The report further states that “that transdermal options carry the lowest risk of VTE for transgender individuals.” Although research on VTE risk in transgender individuals undergoing GAHT continues to evolve, the ASH emphasizes that the increased risk warrants consideration.44
American College of Obstetricians and Gynecologists
The 2013 ACOG clinical management guidelines recommend that screening for inherited thrombophilia “may be considered in the following clinical settings:
- “A personal history of venous thromboembolism that was associated with a non-recurrent risk factor
- A first degree relative (parent or sibling) with a history of high-risk thrombophilia.”45
The 2018 ACOG Practice Bulletin Summary Number 197 supersedes the above 2013 guidelines (Practice Bulletin Number 138). In this update, the ACOG makes the following recommendations regarding screening based on “limited or inconsistent scientific evidence”:
“Screening for inherited thrombophilias is not recommended for women with a history of fetal loss or adverse pregnancy outcomes including abruption, preeclampsia, or fetal growth restriction because there is insufficient clinical evidence that antepartum prophylaxis with unfractionated heparin or low molecular-weight heparin prevents recurrence in these patients.”
“Because of the lack of association between either heterozygosity or homozygosity for the MTHFR C677T polymorphism and any negative pregnancy outcomes, including any increased risk of VTE, screening with either MTHFR mutation analyses or fasting homocysteine levels is not recommended.”
The 2018 ACOG recommends the following screening guideline based on “consensus and expert opinion”:
“Among women with personal histories of VTE, recommended screening tests for inherited thrombophilias should include factor V Leiden mutation; prothrombin G20210A mutation; and antithrombin, protein S, and protein C deficiencies.”46
Evaluation of Genomic Applications in Practice and Prevention
“The Evaluation of Genomic Applications in Practice and Prevention Working Group (EGAPP) found adequate evidence to recommend against routine testing for Factor V Leiden (FVL) and/or prothrombin 20210G>A47 in the following circumstances: (1) adults with idiopathic venous thromboembolism (VTE). In such cases, longer term secondary prophylaxis to avoid recurrence offers similar benefits to patients with and without one or more of these mutations. (2) Asymptomatic adult family members of patients with VTE and an FVL or PT mutation, for the purpose of considering primary prophylactic anticoagulation. Potential benefits are unlikely to exceed potential harms. The evidence was insufficient to determine whether FVL/PT testing might have clinical utility in some circumstances, such as for identifying FVL homozygosity among asymptomatic family members of adults with idiopathic VTE or counseling patients about the risks and benefits of antithrombotic therapy. The recommendations do not extend to patients with other risk factors for thrombosis, such as contraceptive use, as the evidence review that serves as the basis for the recommendations focused primarily on idiopathic VTE.”47
The Anticoagulation Forum
The Anticoagulation Forum published guidelines on the evaluation and treatment of hereditary and acquired thrombophilia in the Journal of Thrombosis and Thrombolysis.1
- “Do not perform thrombophilia testing following an episode of provoked VTE. A positive thrombophilia evaluation is not a sufficient basis to offer extended anticoagulation following an episode of provoked VTE.
- Do not perform thrombophilia testing in patients following an episode of unprovoked VTE. If a patient with unprovoked VTE and low bleeding risk is planning to stop anticoagulation, test for thrombophilia if test results would change this decision. A negative thrombophilia evaluation is not a sufficient basis to stop anticoagulants following an episode of unprovoked VTE in a patient with low bleeding risk and willingness to continue therapy. Heterozygosity for FVL or PGM does not increase the predicted risk of recurrence after unprovoked VTE to a clinically significant degree.
- Do not test for thrombophilia in asymptomatic family members of patients with VTE or hereditary thrombophilia. As a family history of VTE confers an excess risk of thrombosis, relatives should be counseled regarding use of prophylaxis in high-risk situations.
- Do not test for thrombophilia in asymptomatic family members of patients with VTE or hereditary thrombophilia who are contemplating use of estrogen. If an [individual] is contemplating estrogen use has a first-degree relative with VTE and a known hereditary thrombophilia, test for that thrombophilia if the result would change the decision to use estrogen.
- Do not perform thrombophilia testing at the time of VTE diagnosis or during the initial 3-month course of anticoagulant therapy. When testing for thrombophilias following VTE, use either a 2-stage testing approach or perform testing after a minimum of three months of anticoagulant therapy has been completed, and anticoagulants have been held.
- Do not test for thrombophilia in asymptomatic family members of patients with VTE or hereditary thrombophilia who are contemplating pregnancy. If [an individual] contemplating pregnancy has a first-degree relative with VTE and a known hereditary thrombophilia… test for that thrombophilia if the result would change VTE prophylaxis decisions.”1
American College of Cardiology (ACC)
In 2017, guidance published in the New England Journal of Medicine by Gupta, et al. (2017) was summarized by Barnes (2017) for the American College of Cardiology:
- “Venous thromboembolism (VTE) affects an estimated 300,000-600,000 patients annually in the United States.
- The risk of VTE recurrence is best predicted by whether the initial VTE episode was provoked or unprovoked, not the results of inherited thrombophilia testing.
- Most patients with a provoked VTE have recently undergone surgery, immobility, trauma, or have a concurrent cancer diagnosis. Concurrent use of hormones (e.g., estrogen-containing contraceptive pills) is also frequently considered a provoking factor for VTE development.
- For patients with a first provoked VTE event, guidelines recommend anticoagulation for only 3 months (not longer). Prolonged anticoagulation is associated with an increased risk of bleeding that outweighs the risk of VTE recurrence for these patients.
- Patients with an unprovoked VTE (none of the provoking risk factors listed above) require longer anticoagulation due to a higher risk of recurrence that outweighs the risk of bleeding associated with long-term anticoagulation therapy.
- Thrombophilia testing performed in the setting of an acute clot or ongoing anticoagulation therapy will often result in spurious results (usually false positive). For example, natural anticoagulants (e.g., protein C and S, antithrombin) are consumed during an acute thrombotic event and the levels can be reduced by ongoing anticoagulant therapy.
- A recent study identified that up to 55% of Medicare patients with provoked VTE had undergone inappropriate thrombophilia testing, associated with significant cost to the healthcare system.
- While thrombophilia testing rarely impacts management decisions about anticoagulation therapy, it may be beneficial for genetic testing purposes in patients presenting with a first unprovoked VTE at a young age (e.g., <45 years) or at an unusual site.
- For patients with unprovoked VTE at a young age, VTE at an unusual site, arterial thrombosis, or pregnancy morbidity, testing for antiphospholipid antibodies, JAK2 mutation, and paroxysmal nocturnal hemoglobinuria may be beneficial.
- There is no role for extensive cancer screening (e.g., computed tomography scanning) in patients with VTE. Only routine, age-appropriate cancer screening is recommended.”48,49
Again in 2017, key points—inclusive of guiding points—published in the New England Journal of Medicine by Connors (2017) were captured by Barnes (2017) for the ACC:
- “The majority of patients with venous thromboembolism (VTE) should not be tested for thrombophilia. Data supporting clinical usefulness and benefits are limited or nonexistent.
- Most patients with inherited thrombophilia can be identified by coagulation experts based on the patient’s personal and family history of VTE. Thrombophilia testing is usually not required.
- Factors associated with an inherited thrombophilia include VTE at a young age (<40-50 years), a strong family history of VTE, VTE in conjunction with weak provoking factors at a young age, recurrent VTE, and VTE in an unusual site (e.g., cerebral or splanchnic veins).
- Do not perform thrombophilia testing at the time of a VTE event, as it can be inaccurate (often false positive). Perform testing (when indicated) after completion of initial therapy and if it might change management strategies.
- Do not perform thrombophilia testing while a patient is receiving anticoagulation. Instead, wait until two weeks after discontinuing warfarin, or two days for direct oral anticoagulants and heparin.
- The goal of thrombophilia testing should be to aid decision making regarding future VTE prophylaxis, to guide testing of family members, and to determine the cause in severe or fatal VTE. Test results alone should not be used to decide on the duration of anticoagulation therapy.
- Most VTE recurrence risk tools do not incorporate thrombophilia test results into their risk stratification schemes.
- For patients with provoked VTE, even if they have homozygous factor V Leiden, prothrombin gene mutations, or deficiencies of protein S, C, or antithrombin, they do not require lifelong anticoagulation.
- Currently available thrombophilia tests are insufficient to identify inherited risks of VTE. Therefore, a negative test should not be interpreted as a patient being free of thrombophilia.
- Testing for the antiphospholipid antibody syndrome may be useful in patients with unprovoked VTE if there is clinical equipoise about extended anticoagulation courses. It can also be useful to determine warfarin versus direct oral anticoagulant therapy.”13,50
European Society of Cardiology
The ESC has published guidelines for the diagnosis and management of acute PE. These guidelines state:
- “D-dimer measurement and clinical prediction rules should be considered to rule out PE during pregnancy or the post-partum period
- Plasma D-dimer measurement, preferably using a highly sensitive assay, is recommended in outpatients/emergency department patients with low or intermediate clinical probability, or those that are PE-unlikely, to reduce the need for unnecessary imaging and irradiation
- A D-dimer test, using an age-adjusted cut-off or adapted to clinical probability, should be considered as an alternative to the fixed cut-off level
- D-dimer measurement is not recommended in patients with high clinical probability, as a normal result does not safely exclude PE, even when using a highly sensitive assay
- Assessment of the RV [right ventricle] by imaging methods or laboratory biomarkers should be considered, even in the presence of a low PESI [Pulmonary Embolism Severity Index] or a negative sPESI [simplified Pulmonary Embolism Severity Index].”51
In 2021, the ESC Working Group released guidelines on diagnosis and management of acute deep vein thrombosis. These guidelines suggest that “ELISA D-dimer or highly sensitive immunoturbidimetric tests should be measured in ‘unlikely’ clinical probability patients to exclude DVT diagnosis.”52
In 2025, the ESC, in tandem with the European Society of Gynecology (ESG), updated guidelines for management of cardiovascular disease and pregnancy. They recommend that “In pregnant women or women in the post-partum period with suspicion of venous thromboembolism (VTE) (deep vein thrombosis [DVT] and/or PE), an immediate formal diagnostic assessment with validated methods is recommended and should not be postponed.”53 Additionally, they note that “Progestin-only treatment, contraceptive implants, and/or levonorgestrel IUDs should be considered when there is any risk of thromboembolic events.”53
World Health Organization (WHO)
In the WHO medical eligibility criteria for contraceptive use, known thrombogenic mutations (e.g. factor V Leiden; prothrombin mutation; protein S, protein C, and antithrombin deficiencies) are “a condition which represents an unacceptable health risk if the contraceptive method is used” when considering combined hormonal contraceptives, and the method is “not to be used.” The WHO notes that “among women with thrombogenic mutations, COC users had a 2- to 20-fold higher risk of thrombosis than non-users.” When considering progestogen-only contraceptives, intrauterine devices, barrier methods, or female surgical sterilization, known thrombogenic mutations are “a condition for which there is no restriction for the use of the contraceptive method” or “the advantages of using the method generally outweigh the theoretical or proven risks.” In all cases, the WHO clarifies that “routine screening is not appropriate because of the rarity of the conditions and the high cost of screening.”54
National Institute for Health and Care Excellence (NICE)
In the NICE venous thromboembolic disease guidelines, for thrombophilia testing, it is recommended:
- “Do not offer testing for hereditary thrombophilia to people who are continuing anticoagulation treatment.
- “Do not offer thrombophilia testing to people who have had provoked DVT or PE.”
- “Consider testing for antiphospholipid antibodies in people who have had unprovoked DVT or PE if it is planned to stop anticoagulation treatment, but be aware that these tests can be affected by anticoagulants and specialist advice may be needed.”
- “Consider testing for hereditary thrombophilia in people who have had unprovoked DVT or PE and who have a first‑degree relative who has had DVT or PE if it is planned to stop anticoagulation treatment, but be aware that these tests can be affected by anticoagulants and specialist advice may be needed.”
“Do not routinely offer thrombophilia testing to first‑degree relatives of people with a history of DVT or PE and thrombophilia.” 55
American College of Radiology (ACR)
The ACR has guidelines for suspected PE. The ARC prefaced that their publication “focuses on the initial evaluation for clinically suspected PE, recognizing that as many as 80% of PE cases are associated with DVT” and that “PE also may occur without detectable DVT.” The guidelines do not mention any laboratory or genetic testing, although some of the imaging recommendations are based on positive or negative D-dimer results.56
Thrombosis Canada
Thrombosis Canada released guidelines on the diagnosis of PE.⁵⁵ They emphasize that PE signs and symptoms are nonspecific and can overlap with many other conditions. Clinical presentation ranges widely, from mild symptoms to cardiac arrest, making early diagnosis and treatment critical to reduce morbidity and mortality. They also noted that the widespread use of CTPA has led to a significant rise in scans for suspected PE, resulting in more unnecessary imaging and the detection of PEs that have not meaningfully reduced overall mortality, highlighting concerns about overdiagnosis and the clinical relevance of these cases. Recommendations for determining the need for imaging to diagnosis is to use a three step approach.
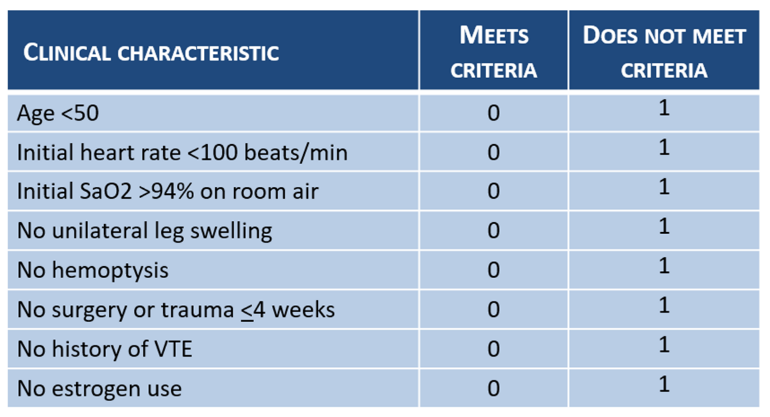
- “Assess the pretest clinical probability (PTP) using a validated clinical prediction rule such as the Wells’ score (Table 1), the Geneva score, or using empiric evaluation. In patients with a low empiric pretest probability of PE and all clinical criteria of the Pulmonary Embolism Rule-out Criteria (PERC, Table 2), no further testing is required, not even D-dimer measurement.
- D-dimer measurement, using a sensitive assay. Given the high sensitivity (greater than 90%) of D-dimer assays resulting in a high negative predictive value, a negative D-dimer rules out PE among patients with a low or moderate (or ‘unlikely’) PTP. Using a sensitive D-dimer assay, the age-adjusted threshold for positivity is >500 mcg/l for patients less than 50 years old and >“age x10” for patients 50 years of age or older.
- Proceed with imaging in patients with a positive D-dimer or high PTP (or ‘likely’). Imaging studies include multidetector CTPA and ventilation-perfusion scans.”57
Table 1: Wells Score* for PE:57
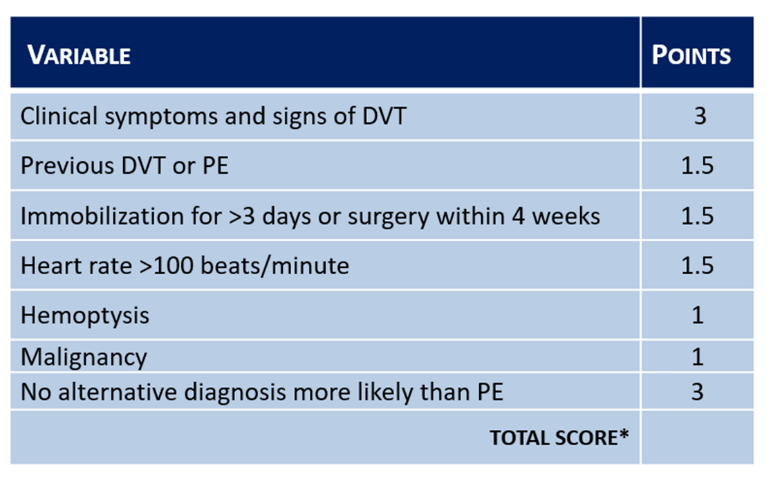
Table 2: PE Rule-out Criteria (PERC) for patients with low pretest probability for PE:57
They also recommend that “patients with suspected DVT should first undergo a history and physical exam focused on the components of the Wells' Score, as well as symptoms and signs of PE.
- Patients with an unlikely PTP for DVT should then undergo D-dimer testing with management as outlined in Figure 1 below.
- Patients with a likely PTP should have either a proximal CUS or whole leg CUS as the recommended first-line test. Those with a negative proximal CUS should undergo D-dimer testing (to determine the need for repeat CUS) and repeat proximal CUS in 5-7 days to exclude the possibility of distal DVT that has extended proximally. Those with a negative whole leg CUS do not require D-dimer or repeat CUS.”58
Figure 1. Suggested diagnostic strategy for patients with suspected DVT:58
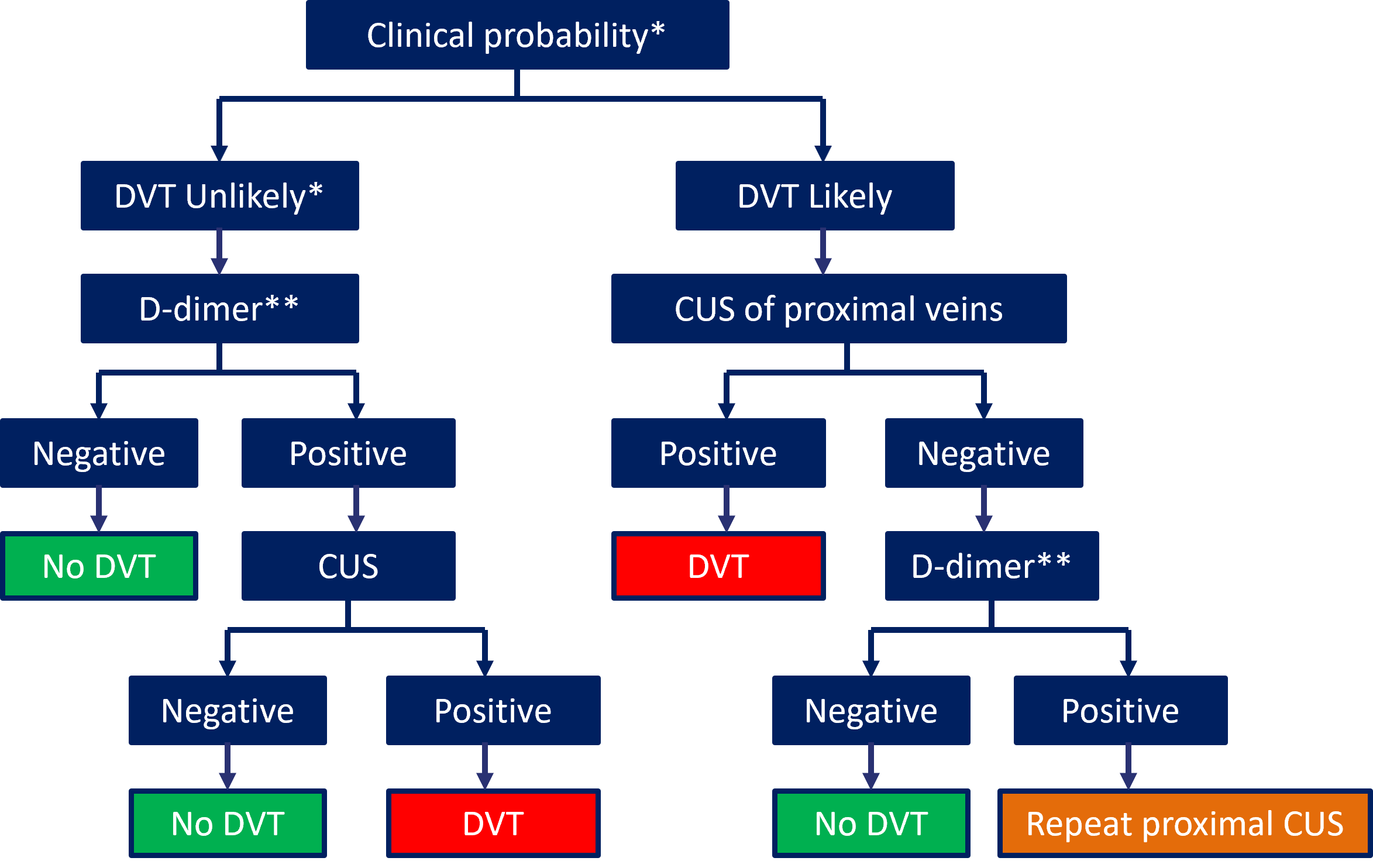
“*Clinical probability can be assessed by clinical decision rule, such as two-level Wells' score.
**D-dimer should be measured using a highly sensitive assay to rule out DVT using this algorithm; if D-dimer testing is not available, CUS should be performed in all patients; a negative CUS and unlikely pre-test probability excludes DVT, while patients with a likely pre-test probability and negative CUS should have CUS repeated in 5-7 days.”58
Thrombosis Canada provides several clinical guidelines addressing conditions related to thrombophilia. Regarding testing for protein C, protein S, or antithrombin (AT), they recommend that “Specialist advice should be sought before considering thrombophilia testing in patients with DVT or PE.” They further state that thrombophilia testing is not recommended for patients who experience venous thromboembolism (VTE) provoked by a strong triggering factor (e.g., major surgery) or for patients with arterial thrombosis. Additionally, thrombophilia testing should not be included as part of broad population screening, and routine testing is not advised prior to starting oral contraceptives, hormone therapy, or for prenatal screening.59
Thrombosis Canada also provides specific recommendations for FVL and prothrombin gene mutation (PGM) testing, advising against using Factor V Leiden and prothrombin gene mutation testing as a screening tool in healthy individuals. Testing may be considered only in limited circumstances, such as asymptomatic women with a first-degree relative with known thrombophilia and a history of VTE who are pregnant, planning pregnancy, or considering hormonal contraception, and only testing when the results would alter decisions regarding thromboprophylaxis or contraceptive choice.60 Regarding pregnant individuals Thrombosis Canada recommends that “If DVT or PE is suspected in the postpartum period, the patient should be investigated as in non-pregnant patients, remembering that the pretest probability will be higher as this is the highest risk time for VTE in pregnant patients.”61
The Endocrine Society
The Endocrine Society published clinical guidance on the endocrine treatment of gender-dysphoric/gender-incongruent persons, which includes emerging evidence regarding the thrombotic risks associated with estrogen therapy in transgender individuals. The guideline notes “VTE may be a serious complication. A study reported a 20-fold increase in venous thromboembolic disease in a large cohort of Dutch transgender subjects. This increase may have been associated with the use of the synthetic estrogen, ethinyl estradiol.”62 Based on these findings, the Endocrine Society recommends that transgender individuals with a family history of VTE undergo thrombophilia testing prior to initiating hormone therapy. The guideline also recommends periodic monitoring of prolactin levels in individuals treated with estrogen. Additionally, clinicians are advised to review estrogen therapy before and after surgical procedures, citing concern that estrogen use may increase the risk of venous thrombosis during the perioperative period or following surgery.”62 They recommend that serum estradiol levels in those receiving estrogen therapy should not exceed the physiological range of 100-200 pg/mL to avoid supraphysiological estradiol concentrations, which has been linked to increasing the risk of VTE.
References
1. Stevens SM, Woller SC, Bauer KA, et al. Guidance for the evaluation and treatment of hereditary and acquired thrombophilia. J Thromb Thrombolysis. 2016;41:154-64. doi:10.1007/s11239-015-1316-1
2. Bartholomew JR. Update on the management of venous thromboembolism. Cleveland Clinic journal of medicine. Dec 2017;84(12 Suppl 3):39-46. doi:10.3949/ccjm.84.s3.04
3. Herrmann J. Clinical Cardio-Oncology. Elsevier; 2018.
4. Bauer KA, Lip GY. Overview of the causes of venous thrombosis in adults. Updated March 18, 2026. https://www.uptodate.com/contents/overview-of-the-causes-of-venous-thrombosis-in-adults
5. Byrnes JR, Wolberg AS. Red blood cells in thrombosis. Blood. Oct 19 2017;130(16):1795-1799. doi:10.1182/blood-2017-03-745349
6. Bauer KA. Clinical presentation and diagnosis of the nonpregnant adult with suspected deep vein thrombosis of the lower extremity. Updated January 16, 2026. https://www.uptodate.com/contents/clinical-presentation-and-diagnosis-of-the-nonpregnant-adult-with-suspected-deep-vein-thrombosis-of-the-lower-extremity
7. Thompson BT, Kabrhel, Christopher. Overview of acute pulmonary embolism in adults. Updated October 09, 2025. https://www.uptodate.com/contents/overview-of-acute-pulmonary-embolism-in-adults
8. Crous-Bou M, Harrington LB, Kabrhel C. Environmental and genetic risk factors associated with venous thromboembolism. Semin Thromb Hemost. Nov 2016;42(8):808-20. doi:10.1055/s-0036-1592333
9. Middeldorp S. Factor V Leiden and activated protein C resistance. Updated April 23, 2025. https://www.uptodate.com/contents/factor-v-leiden-and-activated-protein-c-resistance
10. Bauer KA. Protein S deficiency. Updated December 5, 2025. https://www.uptodate.com/contents/protein-s-deficiency
11. Bauer KA. Prothrombin G20210A. Updated May 30, 2025. https://www.uptodate.com/contents/prothrombin-g20210a
12. Bauer KA. Protein C deficiency. Updated January 29, 2026. https://www.uptodate.com/contents/protein-c-deficiency
13. Connors JM. Thrombophilia Testing and Venous Thrombosis. N Engl J Med. 2017;377(23):2298. doi:10.1056/NEJMc1713797
14. Bauer KA, Stevens SM. Evaluation for thrombophilia and occult malignancy in adults with venous thromboembolism. Updated December 15, 2025. https://www.uptodate.com/contents/evaluation-for-thrombophilia-and-occult-malignancy-in-adults-with-venous-thromboembolism
15. Kujovich JL. Factor V Leiden thrombophilia. Genet Med. Jan 2011;13(1):1-16. doi:10.1097/GIM.0b013e3181faa0f2
16. Carroll BJ, Piazza G. Hypercoagulable states in arterial and venous thrombosis: When, how, and who to test? Vasc Med. Aug 2018;23(4):388-399. doi:10.1177/1358863x18755927
17. Kujovich JL. Factor V Leiden Thrombophilia. In: Adam MP, Ardinger HH, Pagon RA, et al, eds. GeneReviews((R)). University of Washington, Seattle; 2018.
18. Previtali E, Bucciarelli P, Passamonti SM, Martinelli I. Risk factors for venous and arterial thrombosis. Blood Transfus. Apr 2011;9(2):120-38. doi:10.2450/2010.0066-10
19. NATF. Genetic Risk Factors for Blood Clots and the Role of Genetic Testing. Updated July 21, 2022. https://thrombosis.org/patients/patient-articles/genetic-risk-factors-for-blood-clots-and-the-role-of-genetic-testing
20. Raffini L. Thrombophilia testing in children and adolescents. Updated July 15, 2025. https://www.uptodate.com/contents/thrombophilia-testing-in-children-and-adolescents
21. Curtis C, Mineyko A, Massicotte P, et al. Thrombophilia risk is not increased in children after perinatal stroke. Blood. May 18 2017;129(20):2793-2800. doi:10.1182/blood-2016-11-750893
22. Ferriero DM, Fullerton HJ, Bernard TJ, et al. Management of Stroke in Neonates and Children: A Scientific Statement From the American Heart Association/American Stroke Association. Stroke. 2019;50(3)doi:10.1161/str.0000000000000183
23. Lehman LL, Beaute J, Kapur K, et al. Workup for Perinatal Stroke Does Not Predict Recurrence. Stroke. 2017;48(8):2078-2083. doi:10.1161/STROKEAHA.117.017356
24. de Moerloose P, Reber G, Perrier A, Perneger T, Bounameaux H. Prevalence of factor V Leiden and prothrombin G20210A mutations in unselected patients with venous thromboembolism. Br J Haematol. Jul 2000;110(1):125-9. doi:10.1046/j.1365-2141.2000.02039.x
25. Mäkelburg AB, Veeger NJ, Middeldorp S, et al. Different risk of deep vein thrombosis and pulmonary embolism in carriers with factor V Leiden compared with non-carriers, but not in other thrombophilic defects. Results from a large retrospective family cohort study. Haematologica. Jun 2010;95(6):1030-3. doi:10.3324/haematol.2009.017061
26. Murphy CH, Sabath DE. Comparison of Phenotypic Activated Protein C Resistance Testing With a Genetic Assay for Factor V Leiden. Am J Clin Pathol. Feb 4 2019;151(3):302-305. doi:10.1093/ajcp/aqy142
27. Chiasakul T, De Jesus E, Tong J, et al. Inherited Thrombophilia and the Risk of Arterial Ischemic Stroke: A Systematic Review and Meta-Analysis. J Am Heart Assoc. Oct 2019;8(19):e012877. doi:10.1161/jaha.119.012877
28. Ordieres-Ortega L, Demelo-Rodríguez P, Galeano-Valle F, Kremers BMM, ten Cate-Hoek AJ, ten Cate H. Predictive value of D-dimer testing for the diagnosis of venous thrombosis in unusual locations: A systematic review. Thrombosis Research. 2020/05/01/ 2020;189:5-12. doi:10.1016/j.thromres.2020.02.009
29. Linkins LA, Takach Lapner S. Review of D-dimer testing: Good, Bad, and Ugly. Int J Lab Hematol. May 2017;39 Suppl 1:98-103. doi:10.1111/ijlh.12665
30. Algahtani FH, Stuckey R. High factor VIII levels and arterial thrombosis: illustrative case and literature review. Ther Adv Hematol. 2019;10:2040620719886685. doi:10.1177/2040620719886685
31. Bank I, Libourel EJ, Middeldorp S, et al. Elevated levels of FVIII:C within families are associated with an increased risk for venous and arterial thrombosis. J Thromb Haemost. Jan 2005;3(1):79-84. doi:10.1111/j.1538-7836.2004.01033.x
32. Lee EJ, Dykas DJ, Leavitt AD, et al. Whole-exome sequencing in evaluation of patients with venous thromboembolism. Blood advances. Jul 11 2017;1(16):1224-1237. doi:10.1182/bloodadvances.2017005249
33. Segal JB, Brotman DJ, Emadi A, et al. Outcomes of genetic testing in adults with a history of venous thromboembolism. Evidence report/technology assessment. Jun 2009;(180):1-162.
34. Onda S, Furukawa K, Haruki K, et al. d-dimer-based screening for early diagnosis of venous thromboembolism after hepatectomy. Langenbeck's Archives of Surgery. 2021/05/01 2021;406(3):883-892. doi:10.1007/s00423-020-02058-9
35. Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke. Jul 2021;52(7):e364-e467. doi:10.1161/str.0000000000000375
36. Kang BE, Zhang S, Lesmana H, et al. Venous thromboembolism laboratory testing (factor V Leiden and factor II c.∗97G>A), 2025 revision: A technical standard of the American College of Medical Genetics and Genomics (ACMG). Genetics in Medicine. 2025;27(8)doi:10.1016/j.gim.
37. Zhang S, Taylor AK, Huang X, et al. Venous thromboembolism laboratory testing (factor V Leiden and factor II c.*97G>A), 2018 update: a technical standard of the American College of Medical Genetics and Genomics (ACMG). Genet Med. Dec 2018;20(12):1489-1498. doi:10.1038/s41436-018-0322-z
38. Hickey SE, Curry CJ, Toriello HV. ACMG Practice Guideline: lack of evidence for MTHFR polymorphism testing. Genet Med. Feb 2013;15(2):153-6. doi:10.1038/gim.2012.165
39. Bashford MT, Hickey SE, Curry CJ, et al. Addendum: ACMG Practice Guideline: lack of evidence for MTHFR polymorphism testing. Genetics in Medicine. 2020/12/01 2020;22(12):2125-2125. doi:10.1038/s41436-020-0843-0
40. ASH. ASH - Testing for thromboembolism | Choosing Wisely. Choosing Wisely https://www.hematology.org/education/clinicians/guidelines-and-quality-care/choosing-wisely
41. Lim W, Le Gal G, Bates SM, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: diagnosis of venous thromboembolism. Blood advances. 2018;2(22):3226. doi:10.1182/bloodadvances.2018024828
42. Ortel TL, Neumann I, Ageno W, et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood advances. 2020;4(19):4693-4738. doi:10.1182/bloodadvances.2020001830
43. Middeldorp S, Nieuwlaat R, Baumann Kreuziger L, et al. American Society of Hematology 2023 guidelines for management of venous thromboembolism: thrombophilia testing. Blood advances. Nov 28 2023;7(22):7101-7138. doi:10.1182/bloodadvances.2023010177
44. King H, Kelley TP, Shatzel JJ. Gender-affirming hormone therapy in the transgender patient: influence on thrombotic risk. Hematology. 2024;2024(1):652-663. doi:10.1182/hematology.2024000592
45. ACOG. ACOG Practice Bulletin No. 138: Inherited thrombophilias in pregnancy. Obstetrics and gynecology. Sep 2013;122(3):706-17. doi:10.1097/01.AOG.0000433981.36184.4e
46. ACOG. ACOG Practice Bulletin No. 197 Summary: Inherited Thrombophilias in Pregnancy. Obstetrics and gynecology. Jul 2018;132(1):249-251. doi:10.1097/aog.0000000000002705
47. EGAPP. Recommendations from the EGAPP Working Group: routine testing for Factor V Leiden (R506Q) and prothrombin (20210G>A) mutations in adults with a history of idiopathic venous thromboembolism and their adult family members. Genet Med. Jan 2011;13(1):67-76. doi:10.1097/GIM.0b013e3181fbe46f
48. Gupta A, Sarode R, Nagalla S. Thrombophilia Testing in Provoked Venous Thromboembolism: A Teachable Moment. JAMA Internal Medicine. 2017;177(8):1195-1196. doi:10.1001/jamainternmed.2017.1815
49. Barnes G. Thrombophilia Testing for Provoked VTE. American College of Cardiology; 2017;2019(02/13/2019). https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2017/06/05/12/46/thrombophilia-testing-in-provoked-venous-thromboembolism
50. Barnes GD. Thrombophilia Testing and Venous Thrombosis. American College of Cardiology; 2017. https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2017/10/20/11/18/thrombophilia-testing-and-venous-thrombosis.
51. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J. Sep 2019;54(3)doi:10.1183/13993003.01647-2019
52. Mazzolai L, Ageno W, Alatri A, et al. Second consensus document on diagnosis and management of acute deep vein thrombosis: updated document elaborated by the ESC Working Group on aorta and peripheral vascular diseases and the ESC Working Group on pulmonary circulation and right ventricular function. European Journal of Preventive Cardiology. 2022;doi:10.1093/eurjpc/zwab088
53. De Backer J, Haugaa KH, Hasselberg NE, et al. 2025 ESC Guidelines for the management of cardiovascular disease and pregnancy: Developed by the task force on the management of cardiovascular disease and pregnancy of the European Society of Cardiology (ESC)Endorsed by the European Society of Gynecology (ESG). European Heart Journal. 2025;46(43):4462-4568. doi:10.1093/eurheartj/ehaf193
54. WHO. Medical eligibility criteria for contraceptive use: web annex: development of updated recommendations and Grading of Recommendations Assessment, Development and Evaluation (GRADE) tables, 6th ed. https://doi.org/10.2471/B09566
55. NICE. Venous thromboembolic diseases: diagnosis, management and thrombophilia testing. Updated August 2, 2023. https://www.nice.org.uk/guidance/ng158/chapter/Recommendations
56. Kirsch J, Wu CC, Bolen MA, et al. ACR Appropriateness Criteria® Suspected Pulmonary Embolism: 2022 Update. J Am Coll Radiol. Nov 2022;19(11s):S488-s501. doi:10.1016/j.jacr.2022.09.014
57. Thrombosis Canada. Pulmonary Embolism (PE): Diagnosis. Updated April 30, 2025. https://thrombosiscanada.ca/hcp/practice/clinical_guides?language=en-ca&guideID=PULMONARYEMBOLISMDIAGNOSISANDM
58. Thrombosis Canada. Deep Vein Thrombosis: Diagnosis. Updated May 7, 2025. https://thrombosiscanada.ca/hcp/practice/clinical_guides?language=en-ca&guideID=DEEPVEINTHROMBOSISDIAGNOSIS
59. Thrombosis Canada. Thrombophilia: Deficiencies in Protein C, Protein S and Antithrombin. Updated November 10, 2025. https://thrombosiscanada.ca/hcp/practice/clinical_guides?language=en-ca&guideID=DEFICIENCIESINPROTEINCPROTEINS
60. Thrombosis Canada. Thrombophilia: Factor V Leiden and Prothrombin Gene Mutation. Updated April 30, 2025. https://thrombosiscanada.ca/hcp/practice/clinical_guides?language=en-ca&guideID=THROMBOPHILIAFACTORVLEIDENANDP
61. Thrombosis Canada. Pregnancy: Diagnosis of DVT and PE. Updated January 6, 2026. https://thrombosiscanada.ca/hcp/practice/clinical_guides?language=en-ca&guideID=83
62. Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism. 2017;102(11):3869-3903. doi:10.1210/jc.2017-01658
Coding Section
| Code |
Number |
Description |
| CPT |
81240 |
F2 (prothrombin, coagulation factor II) (e.g., hereditary hypercoagulability) gene analysis, 20210G>A variant |
|
|
81241 |
F5 (coagulation factor V) (e.g., hereditary hypercoagulability) gene analysis, Leiden variant |
|
|
81291 |
MTHFR (5,10-methylenetetrahydrofolate reductase) (e.g., hereditary hypercoagulability) gene analysis, common variants (e.g., 677T, 1298C) |
|
|
81400 |
Molecular pathology procedure, Level 1 (e.g., identification of single germline variant [e.g., SNP] by techniques such as restriction enzyme digestion or melt curve analysis) |
|
|
81479 |
Unlisted molecular pathology procedure |
|
|
85300 |
Clotting inhibitors or anticoagulants; antithrombin III, activity |
|
|
85301 |
Clotting inhibitors or anticoagulants; antithrombin III, antigen assay |
|
|
85302 |
Clotting inhibitors or anticoagulants; protein C, antigen |
|
|
85303 |
Clotting inhibitors or anticoagulants; protein C, activity |
|
|
85305 |
Clotting inhibitors or anticoagulants; protein S, total |
|
|
85306 |
Clotting inhibitors or anticoagulants; protein S, free |
|
|
85307 |
Activated Protein C (APC) resistance assay |
|
|
0278U |
Hematology (genetic thrombosis), genomic sequence analysis of 14 genes, blood, buccal swab, or amniotic fluid |
| 0529U | Hematology (venous thromboembolism [VTE]), genome-wide single-nucleotide polymorphism variants, including F2 and F5 gene analysis, and Leiden variant, by microarray analysis, saliva, report as risk score for VTE (This code will be effective 01/01/2025) |
| ICD-10-CM | Investigational for all relevant diagnoses | |
| D68.51 | Activated protein C resistance (includes Factor V Leiden mutation) | |
| D68.52 | Prothrombin gene mutation | |
| D68.59 | Other primary thrombophilia | |
| D68.61-D68.69 | Other thrombophilia (includes other hypercoagulable states) | |
| I21.9 (effective 1/1/2018) | Acute myocardial infarction, unspecified | |
| I21.A1 (1/1/2018) | Myocardial infarction on type 2 | |
| I21.A9 (1/1/2018) | Other myocardial infarction type | |
| I26.93 (EFFECTIVE 10/01/2019) | Single subsegmental pulmonary embolism without acute cor pulmonale |
|
| I26.94 (EFFECTIVE 10/01/2019) | Multiple subsegmental pulmonary emboli without acute cor pulmonale | |
| I80.41 -I80.259 (EFFECTIVE 10/01/2019) | Phlebitis and thrombophlebitis of peroneal and calf muscular veins | |
| I82.451 - I82.469 (EFFECTIVE 10/01/2019) | Acute embolism and thrombosis of peroneal and calf muscular veins | |
| I82.551 - I82.569 (EFFECTIVE 10/01/2019) | Chronic embolism and thrombosis of peroneal and calf muscular veins | |
| 087.1 | Deep phlebothrombosis in the puerperium | |
| O87.2 | Hemorrhoids in the puerperium | |
| O87.3 | Cerebral venous thrombosis in the puerperium | |
| O87.4 | Varicose veins of lower extremity in the puerperium | |
| O87.8 | Other venous complications in the puerperium | |
| O87.9 | Venous complication in the puerperium, unspecified | |
| ICD-10-PCS (effective 10/01/15) | Not applicable. ICD-10-PCS codes are only used for inpatient services. There are no ICD procedure codes for laboratory tests. |
Procedure and diagnosis codes on Medical Policy documents are included only as a general reference tool for each policy. They may not be all-inclusive.
This medical policy was developed through consideration of peer-reviewed medical literature generally recognized by the relevant medical community, U.S. FDA approval status, nationally accepted standards of medical practice and accepted standards of medical practice in this community, and other nonaffiliated technology evaluation centers, reference to federal regulations, other plan medical policies, and accredited national guidelines.
"Current Procedural Terminology © American Medical Association. All Rights Reserved"
History From 2014 Forward
| 05/26/2026 | Annual review, removing indication for myocardial infarction as thrombophilia risk testing and updating policy for clarity and consistency. Also updating description, removing assays for clotting inhibitors from note 1, table of terminology, rationale, and references. |
| 04/15/2025 | Annual review, updaing coverage criteria. Also updating rationale and references. |
| 11/13/2024 | Updated Coding Section. Added code 0529U with an effective date of 01/01/2025. No other changes made. |
| 10/14/2024 | Annual review, updating policy to include pulmonary embolism in criteria 1a and creating a new criteria criteria #3 to address known Factor V Leiden or prothromin gene G20210A coverage criteria. Also updating table of terminology, rationale, and references. Also updating verbiage for code 0278U. |
| 07/29/2024 | Change review date to 10/01/2024. |
| 04/25/2024 | Moving review date to 7/2024. Review will coinside with Avalon's review date. |
| 04/12/2023 | Annual review, updating policy for clarity and consistency coverage position for activated protein C (aPC) added. Also updating description, rationale and references. Added notes under policy section. |
| 04/21/2022 |
Annual review, adding criteria #4. Updating rationale, references and coding. Adding table of terminology. |
| 04/22/2021 |
Annual review, updating policy for clarity related to deep vs superficial thrombosis.Also updating description, rationale and references. |
| 04/15/2020 |
Annual review, updating title to include arterial thrombosis and updating medical criteria to address venous testing pre transplant and arterial thrombosis testing. |
| 09/24/2019 |
Updated coding. No other changes made. |
| 04/01/2019 |
Annual review, updating title to reflect scope of testing being addressed. No change to policy intent. |
| 04/19/2018 |
Annual review, updating policy to include medical necessity criteria for Factor V Leiden and G20210A and protein C deficiency, protein S deficiency and antithrombin III deficiency. |
| 09/28/2018 |
Updated policy with 2018 coding. No other changes. |
| 04/26/2017 |
Annual review, no change to policy intent. Updated policy to laboratory category. |
| 11/07/2016 |
Interim review, updating policy verbiage for clarity & specificity of specific testing. |
| 04/13/2016 |
Annual review, no change to policy intent. Updating background, description, rationale and references. |
| 04/11/2016 |
Added CPT code 85307. |
| 01/06/2016 |
Updated CPT codes. No change of the intent of policy. |
| 04/08/2015 |
Annual review, no change to policy intent. Updated regulatory status, rationale and references. Added guidelines, benefit applications and coding. |
| 04/03/2014 |
Annual review. Added related policy and updated references. No change to policy intent. |